Feature images by OpenStax College – Anatomy & Physiology, Connexions Web site. http://cnx.org/content/col11496/1.6/, Jun 19, 2013., CC BY 3.0, Link
This note will describe the anatomical segments of the thoracic aorta, their variants, and some important considerations.
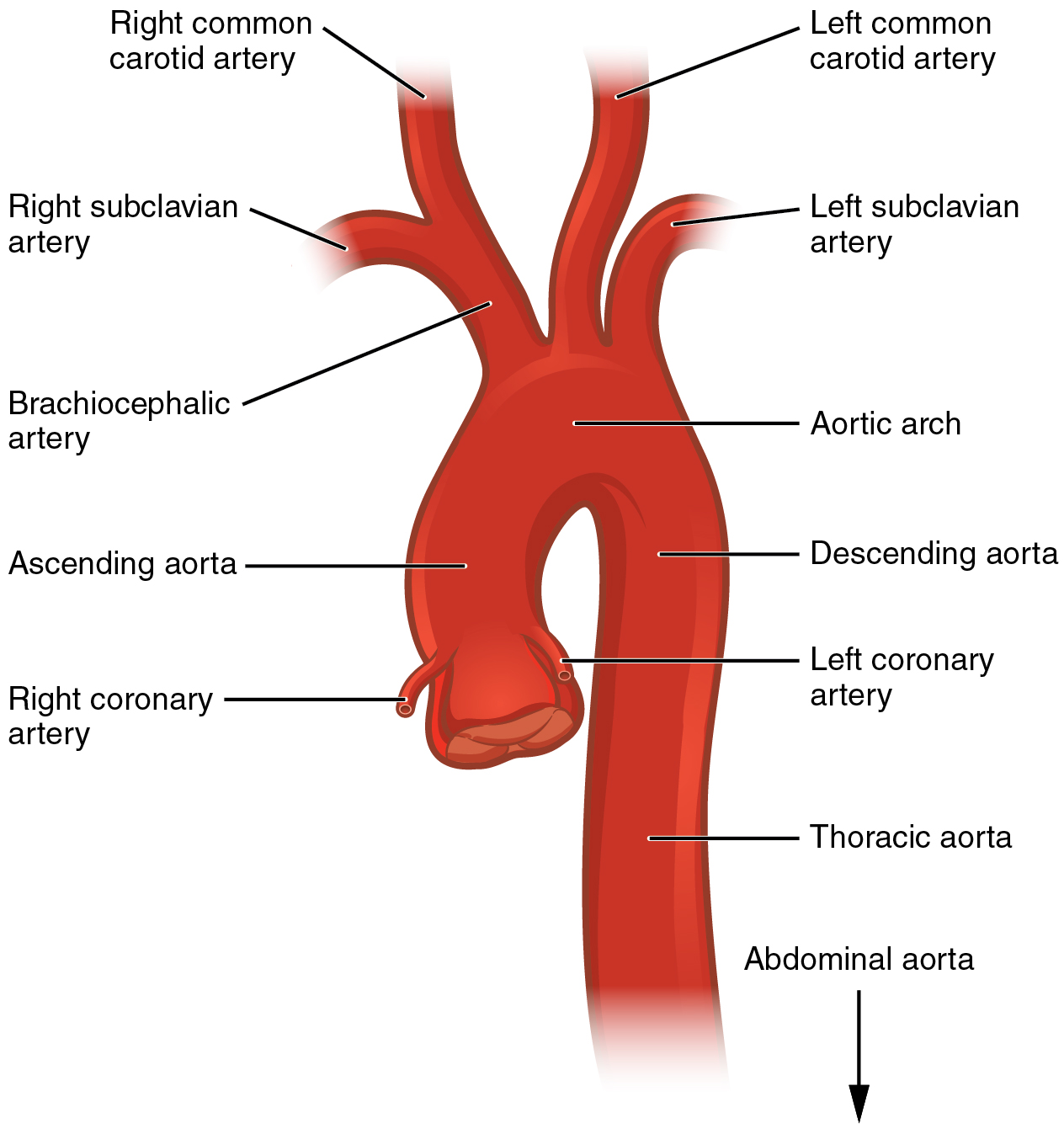
Thoracic aorta has 4 segments from proximal to distal from the heart
Aortic root
Aortic anulus
- Virtual ring defined by lowest attachment point of aortic cusps; typically elliptical shape
- Important for sizing of aortic valve replacement (can be measured pre-operatively with CTA whole aorta)
Sinus of venosus
Typically, it is the greatest caliber segment of the thoracic aorta. There are normally 3 sinuses defined by coronary origins.
- Left main coronary artery (LCM) arises from left coronary sinus
- Right coronary artery (RCA) arises from right coronary sinus
- Interatrial septum points toward noncoronary sinus
Sinotubular junction (STJ)
This is an anatomical landmark dividing the aortic root from the ascending aorta.
Ascending aorta
Extends from STJ to origin of brachiocephalic trunk.
- Typical greatest in diameter and nearly orthogonal to the axial plane at the right pulmonary artery level (which makes it convenient and standard level of measurement).
Aortic arch
Extends from brachiocephalic trunk to ligamentum arteriosum. It is normally “left” sided (continue toward the left).
Normal branching (~75%)
There are normally 3 branches aortic arch branch.
Brachiocephalic trunk (innominate artery)
Divided into
- Right subclavian artery (Right SCA)
Gives off- right internal mammary
- right vertebral artery (right VA)
- right thyrocervical artery
- right costocervical artery
- right long thoracic artery
- continues as right axillary artery after margin of the 1st rib
- Right common carotid artery (Right CCA)
In infants, the large thymus can occasionally cause the normal innominate artery to press against the anterior trachea, potentially producing innominate artery syndrome (a controversial breathing difficulty condition).
Left common carotid artery (Left CCA)
Left subclavin artery (Left SCA)
Gives off branches like its right SCA counterpart.
Variant aortic arch branching
Bovine arch (~20%)
= Common origin of the brachiocephalic artery and left common carotid artery.
4-vessel arch (~5%)
= Left vertebral artery is the third aortic branch, proximal to the left subclavian artery.
Thyroid ima artery (~3%)
The inferior thyroid artery typically arises from the thyrocervical trunk. However, in some cases, it may originate directly from the aortic arch or the innominate artery (in which case it is called the thyroid ima artery). This variation may complicate surgeries in this area, such as thyroidectomy, if not identified pre-operatively.
Aberrant right subclavian (~1%)
= The right subclavian artery arises directly from the aortic arch distal to the left subclavian artery and loops behind the esophagus.
Kommerell diverticulum is a small bulge at the origin of the aberrant subclavian artery. This is mostly an incidental finding and rarely causes symptoms. However, when it compresses the esophagus and causes difficulty swallowing, it is termed dysphagia lusoria. A barium esophagogram will show a posterior indentation on the esophagus.
It is also important to identify the unusual location of the recurrent laryngeal nerve before thyroid surgery to avoid complications.
Vascular rings and sling
These are mostly seen in pediatric populations. It may causes stridor in infancy and childhood that does not explained by more common causes such as infection.
A cheap and effective tool to “screen” this condition is your usual frontal chest film as it may demonstrate a right-sided aortic arch.
Double aortic arch
The most common vascular ring. The arches encircle both the trachea and esophagus. The right arch is usually superior and larger than the left arch. It is arises from 3rd rather than 4th branchial arch and may have anomalous great vessels origins.
The goal of detailed pre-surgical imaging is to determine which arch is dominant, as the non-dominant arch will be ligated to alleviate stridor.
Right arch with aberrant left subclavian artery (non-mirror branching)
In contrast to a “normal” left arch with an aberrant right subclavian artery, which is typically asymptomatic, this variant forms a vascular ring as it is completed by the ligamentum arteriosum. Unlike the mirror-branching subtype, this variant is much less frequently associated with congenital heart disease.
A barium esophagogram cannot reliably distinguish between a double aortic arch and this condition. Therefore, CT or MRI are necessary for a definitive diagnosis after abnormal barium study.
Pulmonary sling
= anomalous origin of the left pulmonary artery arising from the right pulmonary artery coursing between the trachea and esophagus.
Normally only the trachea is trapped, but occasuionally the bronchus intermedius may also be compressed.
This is the only vascular cause of stridor in a patient with a left aortic arch.
Aortic isthmus
The short distal arch segment (~2 cm) betweeen left subclavian artery origin and ligamentum arteriosum. It is typically narrower than adjacent aortic segments.
Ductus diverticulum is focal smooth bulge along undersurface of the aortic isthmus. It is the site of obliterated ductus arteriosus. It is common variant which can be mistaken for traumatic aortic injury, which also frequently occurs at this location. It is considered to be aneurysmal when larger than 3 cm.
Ductus arteriosus
Descending aorta
Extends from distal arch to diaphragmatic hiatus, where it continues as abdominal aorta.
Aortic spindle is bulge in proximal descending aorta just distal to isthmus, more commonly seen in children.
Give offs
- Bronchial arteries (at levels of T4-T5)
- Intercostal arteries
- Supreme intercostals supply T1-T3; arise from costocervical trunk of SCAs
- Paired intercostals arise directly from T4-T12
- Thoracic spinal cord
- Anterior spinal artery is supplied from intercostal and brochial arteries at T4-T5
- Artery of Adamkiewicz arises from intercostal arteries at T6-T12
- Mediastinal branches including
- Esophageal
- Pericardial
- Superior phrenic
Leave a Reply