What is it?
Retrograde urine flow from the bladder toward the kidneys.
What is its importance?
It is usually discovered during the work-up of febrile UTIs in children. There are causal relationships between higher-grade and longer-standing VUR with more frequent UTIs and subsequent renal scarring. The renal scarring, in turn, can cause renal insufficiency, hypertension, and may progress to end-stage renal disease.
Diagnosing this condition in children with a history of UTIs may lead to management strategies that prevent recurrence of UTIs, renal scarring and their complications.
VUR is also associated with other abnormalities of the KUB system, including multicystic dysplastic kidney, ectopic kidney, and duplicated collecting systems.
Trivia
Sterile reflux: associated with renal scarring, as antibiotic prophylaxis after the first UTI reduces the recurrence of febrile UTIs but not scarring.
Ectopic kidney: VUR most commonly involves contralateral orthotopic kidney.
Duplicated collecting systems: Upper pole moiety obstructs while lower pole moiety refluxes.
Is this a common problem?
It is relatively common problem in children, affecting up to 2% of the general pediatric population. It is significantly more frequently seen in children with acute pyelonephritis (25-40%) and in asymptomatic siblings of children with documented reflux (5-50%).
White children are much more commonly affected than Black children, with a ratio ranging from 3:1 to 20:1. Females are more commonly affected than males, with a female-to-male ratio of 2:1.
There are two types of VUR. The first type is primary VUR, which is seen in children and is presumably due to the underdevelopment of the ureter’s insertion into the bladder. It may be too short or abnormally angled compared to adults. The vast majority of children (80%) outgrow this condition before puberty, likely due to the maturation of the ureterovesical junction.
VUR can also be secondary to various causes, including periureteral diverticula, ureterocele, bladder outlet obstruction (most commonly due to BPH), voiding dysfunction, a duplicated collecting system, or neurogenic bladder. Secondary VUR can present in all age groups.
OK, so how is it diagnosed?
As per definition, it is the retrograde flow of urine toward the kidneys. You can visualize it by introducing a contrast agent into the urinary bladder; if you see the contrast above the bladder level, that indicates the presence of reflux.
There are three ways to image this condition: voiding cystourethrogram (VCUG), contrast-enhanced retrograde urosonography (CEUS cystogram), and nuclear cystogram. All these techniques require instilling a contrast agent via bladder catheterization. Which method is best remains controversial. However, understanding the advantages and disadvantages of each is useful.
More facts about pediatrics KUB imaging can be found here.
VCUG
This technique involves the visualization of refluxed iodinated contrast agents via fluoroscopy.
Advantages
Can detect causative pathology with multi-stage images.
- Scout: urolithiasis
- Early filling: intraluminal abnormalities
- Ureterocele
- Polyp
- Mass
- Oblique of distended bladder
- Periureteral diverticula
- Ureteric insertion site
- Voiding: distal pathology
- Posterior urethral valve
- Delayed upright: assess concomitant UPJ or UVJ obstruction (in case of high-grade VUR.)
Disadvantages
- Cannot visualized ectopic ureters that insert below bladder neck (which only reflux during voiding)
- Historically, it had a much higher radiation dose (x100) compared to nuclear cystogram. However, this is no longer true with current pulsed, low-dose fluoroscopy units.
Nuclear cystogram
This technique involves continuously detecting gamma rays from instilled Tc-99m pertechnetate, a radiotracer.
Advantages
- ?
Disadvantages
- Grade I VUR is harder to visualized.
- No information about urethral abnormalities.
CEUS cystogram
Advantages
- No radiation dose.
- Urethral evaluation is possible with US probe on perineum.
- Can look for signs of renal scarring
- Globally small kidney
- Foci of cortical thinning subtended by dilated calyces.
Disadvantages
- Not widely available?
I have heard about VUR grading. Just put it here please.

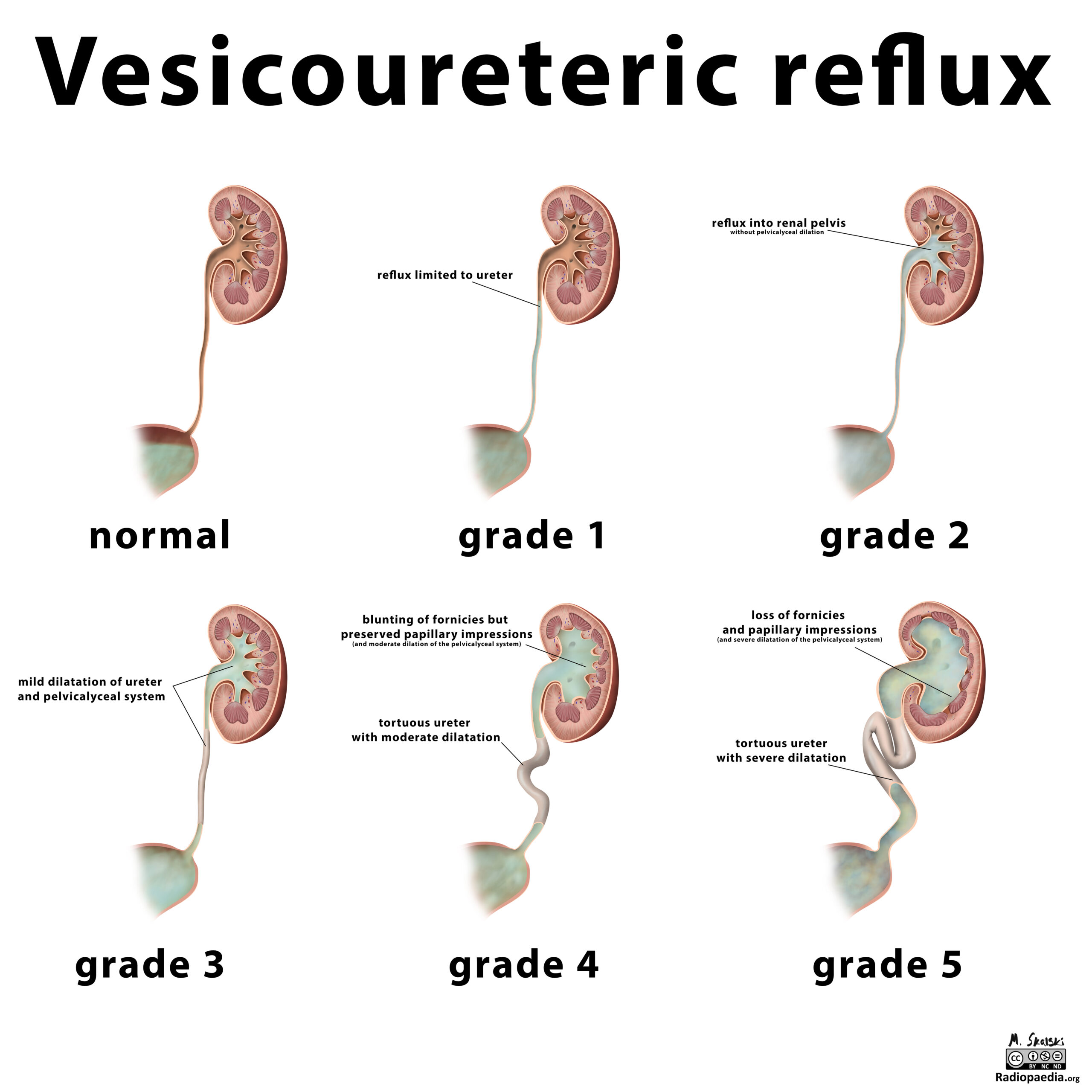
International Reflux Study Committee grading system
I: Reflux into ureter but not reaching renal pelvis
II: Reflux reaching pelvis without blunting of calyces
III: Mild calyceal blunting
IV: Progressive calyceal & ureteral dilation
V: Very dilated & tortuous collecting system
Any grade may include the “intrarenal reflux” modifier, which is associated with increased renal scarring.
How is it treated?
Medical management
Prophylactic antibiotic therapy is used in low-grade reflux to reduce the incidence of febrile UTIs, but as previously mentioned, it does not prevent renal scarring.
Surgical management
Ureteral reimplantation surgery can reduce reflux and subsequent renal scarring.
Minimally invasive management
Use of various inert material to alter shape of refluxing UVJ.
Leave a Reply