Anatomy and function
Together with posterior cruciate ligament (PCL), they are intracapsular but extrasynovial knee joint ligaments (due to coverage by synovial lining).
It originates from the medial margin of the lateral femoral condyle at intercondylar notch, courses anteromedioinferiorly to attach at the anterior tibial plateau, directly lateral to the tibial spine.
Major stabilizer of the knee against anterior tibial translation.
Remain taut throughout the range of knee motion.
Part at tibial attachment is stronger than femoral origin.
Composed of two fiber bundles
- Anteromedial band (smaller but more dominant) → resists anterior tibial subluxation in knee flexion
- Posterolateral band (larger but less dominant) → resists anterior tibial subluxation in knee extension
Interesting facts
The ACL is the most commonly completely tear ligament of the knee. It is also common indication for MRI of the knee.
Mucoid degeneration
- possibly age-related degenerative change
- celery stalk appearance.
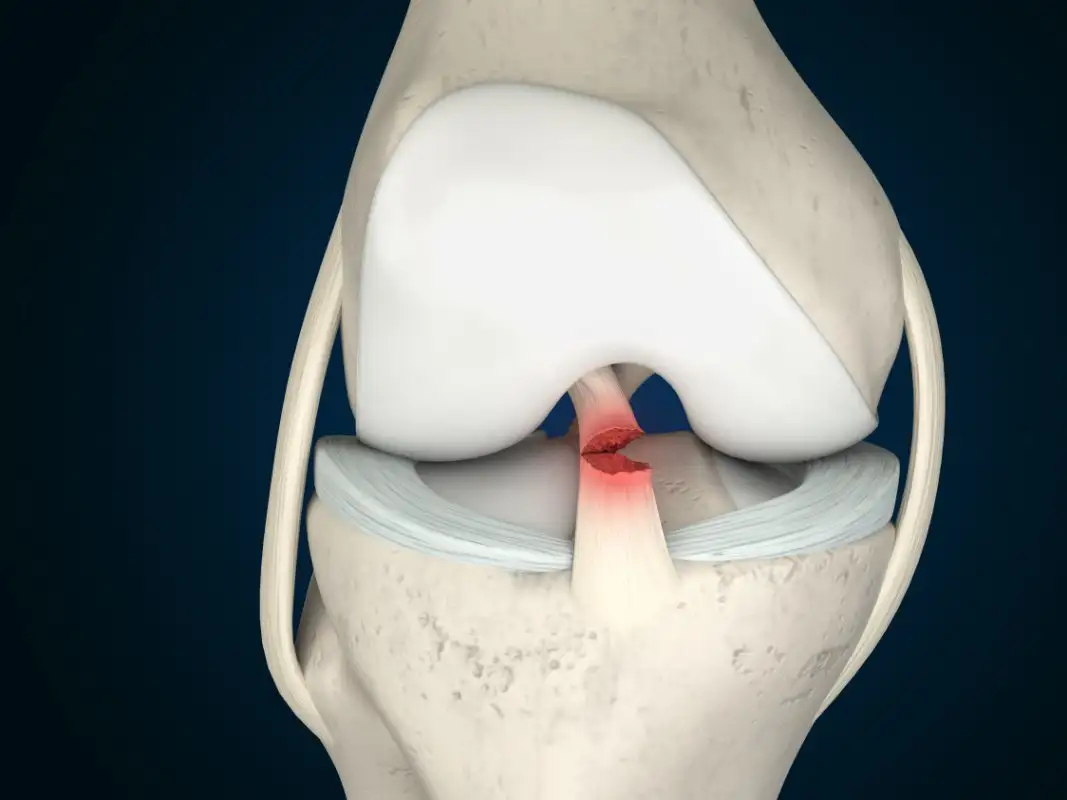
ACL tear
Typically caused by acute injury with mostly either pivot shift or hyperextension mechanism. Usually associated with secondary findings (absent of secondary findings = more likely mucoid degeneration).
Primary signs
As of any ligament in the body, there are three signs of ACL tear on MRI. Best seen in T2WI FS.
- ligament edema
- fiber discontinuity
- change in the expected ligament course
- Normally the ACL fibers are aligned parallel to or slightly steeper than the roof of the intercondylar notch (Blummensaat line)
The most common location of ACL tear is at midportion (= midsubstance). Second most common location is at femoral attachment.
Distal ACL injuries are rare, typically seen in skeletally immature, usually consists of avulsion fractures from the tibial spines.
These primary signs have accuracy more than 90% for ACL evaluation.
Common pitfalls are
- not evaluate in all three planes
- False negative: Sagittal images can miss ligament detachment from the femur
- False positive: Partial volume effect
Pivot shift mechanism
The most common mechanism for ACL tear.
The femur rotate externally on the planted leg (soccer got step on foot).
MCL is the center of rotation creating shear injury at the medial meniscus attachment to the posterior capsule → peripheral vertical tears including ramp lesion, or more severely bucket handle tears.
The lateral femoral condylar surface near the sulcus terminalis impacts on the posterolateral tibia → radial and complex tears of posterior horn of lateral meniscus.
Additional valgus force may cause medial collateral ligament (MCL) injury.
O’Donoghue’s triad = ACL tear + meniscal tears + MCL tears
= Unhappy (medial) triad or terrible triad
Hyperextension mechanism
Can occur upon landing from a jump.
Anterior femoral condyle impacts on the anterior tibial plateau
Distraction at the posterior knee joint → ACL with/without PCL tear + posterior capsular tear
Can result in tibiofemoral dislocation → injury to popliteal vascular structures
Additional varus distraction can cause posterolateral corner injury
Secondary findings
Anterior tibial subluxation
- Anterior drawer sign → line along posterior margin of the lateral tibial plateau lie relatively anterior to the posterior margin of the lateral femoral condyle > 5 mm
- Buckling of the PCL → line of posterior margin of the PCL fail to intersect the femur
- Lateral meniscal uncovering → posterior displacement of peripheral margin of the posterior horn of the lateral meniscus relatively with posterior margin of lateral tibial plateau → loss contact with tibia
- LCL sign → LCL is visualised on coronal images only for one slice. (Normally, we should see more than one due to vertical oblique course of LCL)
Bone bruises
- Impaction from a pivot-shift mechanism causing subchondral bone bruises at the lateral femoral condyle and the posterior lateral tibial plateau
- Posterior margin of medial tibial plateau can also be affected.
However, in pediatric patients bone bruise pattern can occur in the absence of an ACL tear due to greater laxity of the ACL.
Hemarthrosis
Segond fracture
- = avulsion of lateral tibial plateau due to detachment of the lateral capsular ligament. Also seen in iliotibial band injury (insertion on Gerdy’s tubercle of the tibia)
Post ACL reconstruction
ACL graft should run parallel to the intercondylar notch, behind Blumensaat’s line.
- Too steep → impingement with leg extension
- Too lax → knee joint laxity
Leave a Reply